(866) 567-3138
Sponsored Helpline
Verify Insurance
Methocarbamol is a muscle relaxant prescribed to treat muscle pain and spasms. Methocarbamol addiction develops when individuals misuse the drug, taking it in higher doses or using it for longer than prescribed. This leads to physical and psychological dependence, where the user craves its sedative effects, leading to compulsive use. Methocarbamol is not classified as an opioid even though it has a risk of psychological dependency.

Methocarbamol is a muscle relaxant prescribed to treat muscle pain and spasms. Methocarbamol addiction develops when individuals misuse the drug, taking it in higher doses or using it for longer than prescribed. This leads to physical and psychological dependence, where the user craves its sedative effects, leading to compulsive use. Methocarbamol is not classified as an opioid even though it has a risk of psychological dependency.
Methocarbamol abuse has become more prevalent increasing three fold in long-term usage between 2005 and 2016. While new prescriptions remained stable at around 6 million annually, office visits for ongoing therapy jumped from 8.5 million to 24.7 million. Notably, older adults made up 22.2% of these visits in 2016, surpassing their 14.5% representation in the population according to Penn Medicine, in "Long-term Use of Muscle Relaxants Has Skyrocketed Since 2005". Methocarbamol is not classified as a controlled substance by the U.S. Drug Enforcement Administration (DEA). Although it has a low potential for abuse and addiction, its use carries risks, particularly for individuals with a history of substance use disorders.
Signs of methocarbamol addiction include noticeable behavioral changes. People who are addicted to methocarbamol begin taking larger doses than prescribed and engage in "doctor shopping" to acquire additional prescriptions. They withdraw from social activities, neglect personal and professional responsibilities, and take risks to obtain the drug. Increased tolerance is a key sign, as users require higher doses to achieve the same effects.
Methocarbamol addiction leads to a range of physical and psychological symptoms. Physically, users experience drowsiness, dizziness, and confusion due to the drug’s sedative properties. Long-term use results in cognitive impairment, memory issues, and impaired motor coordination. Psychologically, individuals experience cravings, anxiety, depression, and an inability to stop using methocarbamol despite its harmful impact on their lives. Combining methocarbamol with other substances is dangerous. Nearly half of users experience side effects from muscle relaxants, primarily dizziness and sedation according to Daniel J. Mazanec and Russell C. DeMicco’s 2017 Benzel’s Spine Surgery, 2-Volume Set.
Withdrawal from methocarbamol results in symptoms such as anxiety, insomnia, muscle aches, nausea, irritability, and heightened sensitivity to pain. The body experiences these reactions as it adjusts to functioning without the drug. Users also experience headaches, tremors, and restlessness during the withdrawal process.
Treatment for methocarbamol addiction requires a structured approach, beginning with medically supervised detox to manage withdrawal symptoms safely. After detox, behavioral therapies like cognitive-behavioral therapy (CBT) address the underlying reasons for addiction and provide strategies for relapse prevention. Depending on the severity of the addiction, inpatient or outpatient rehabilitation programs offer comprehensive support for long-term recovery.
Methocarbamol addiction is the compulsive use of methocarbamol (Robaxin), a medication classified as a skeletal muscle relaxant. This drug is typically prescribed to alleviate muscle pain and spasms, but when used inappropriately—such as in higher doses or for prolonged periods—it leads to psychological dependence. Methocarbamol is not classified as a controlled substance by the U.S. Drug Enforcement Administration (DEA), and it is considered to have a lower potential for abuse compared to other muscle relaxants, opioids, or benzodiazepines. Individuals with a history of substance use disorders are more prone to misusing methocarbamol due to its sedative properties.
Methocarbamol has a low risk for physical dependence but psychological addiction is possible when the drug is taken beyond its prescribed purpose. Misuse arises from attempting to intensify its sedative effects or combining it with other substances, such as alcohol, which is dangerous. While skeletal muscle relaxants are used less often than medications like pain relievers, they remain a significant concern in the U.S. In 2011, an estimated 53,000 emergency department visits were attributed to the misuse or abuse of muscle relaxants, with 18% involving alcohol, according to Witenko et al.'s 2014 study, “Considerations for the Appropriate Use of Skeletal Muscle Relaxants for the Management of Acute Low Back Pain” . The study also revealed that 44.5% of individuals used muscle relaxants for over a year, despite recommendations for short-term use only.
The misuse of methocarbamol leads to increased tolerance, cravings, and a growing inability to control intake. Over time, this addiction disrupts daily functioning and presents serious health risks, making it important to recognize and address methocarbamol misuse before it escalates into severe dependency.
Methocarbamol, a centrally acting muscle relaxant, is typically used to relieve muscle pain and discomfort associated with acute musculoskeletal conditions. It works by depressing the central nervous system (CNS), which helps reduce muscle spasms without directly affecting the muscles themselves.
The usual initial dosage for adults is 1500 mg, taken three to four times daily. The initial dosage is achieved by taking two 750 mg tablets per dose. For severe conditions, the dosage is increased up to 7500 mg per day, but the dose is generally reduced after the first 48 to 72 hours of treatment to maintain around 4000-4500 mg per day according to “Methocarbamol (Oral Route)” published by the Mayo Clinic. It's important to follow a healthcare provider’s instructions for proper use
The signs, symptoms and side effects of methocarbamol are neurological, gastrointestinal, respiratory, musculoskeletal and severe allergic reactions. These effects become more severe depending on the dosage or severity of the misuse.

The signs, symptoms and side effects of methocarbamol are detailed below:
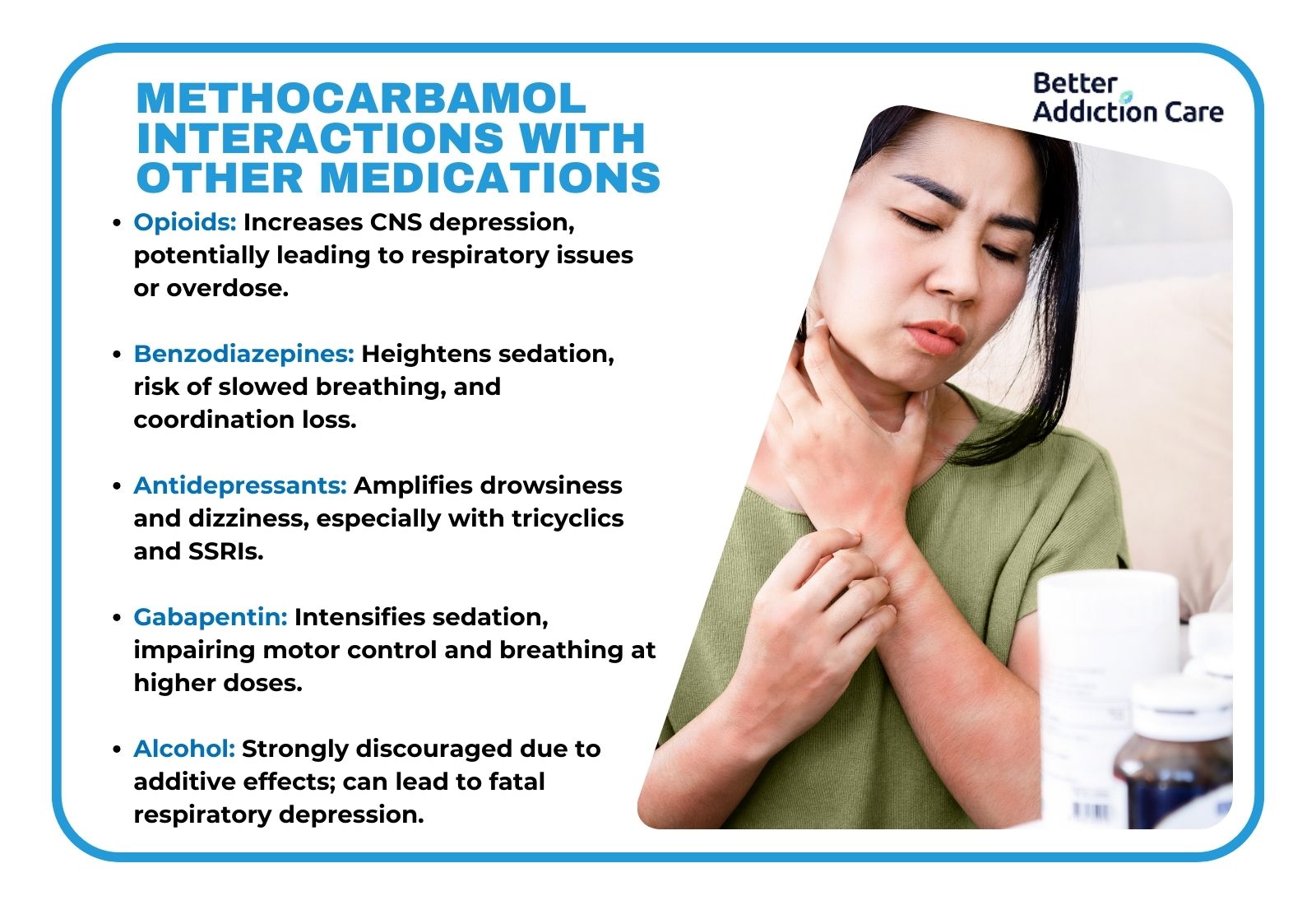
Methocarbamol consumption causes addiction when it is misused. Misuse occurs when individuals take the medication in higher doses or for longer periods than prescribed, seeking its sedative effects. The risk of addiction significantly increases when methocarbamol is combined with other central nervous system (CNS) depressants such as alcohol, opioids, or benzodiazepines. These combinations enhance the drug’s depressant effects, increasing the likelihood of dependence. Regular misuse of methocarbamol, particularly over several weeks, increases the likelihood of developing dependence. While there is no exact timeline for addiction, prolonged misuse—especially when methocarbamol is used in excessive amounts beyond the recommended 6 to 8 grams per day—raises the risk significantly.
Individuals with a history of substance abuse are particularly at risk of developing methocarbamol addiction. Their past misuse of substances makes them more susceptible to seeking similar effects from methocarbamol, especially when used inappropriately or in combination with other CNS depressants. Prolonged misuse leads to both psychological dependence and the compulsive need to continue using the drug despite negative consequences.
The withdrawal timeline for methocarbamol typically begins around 72 hours after the last dose, with symptoms peaking within the first few days. The duration of withdrawal varies depending on factors like dosage, duration of use, and individual differences. In most cases, withdrawal symptoms last from a few days up to two weeks. The acute withdrawal phase tends to resolve within one week, but psychological symptoms, such as anxiety or cravings, persist for a longer period. Withdrawal symptoms are minimal when methocarbamol is taken as prescribed. Pain returns within one to two hours after stopping the medication as its effects wear off according to Ferarra, D. in “Methocarbamol Withdrawal – What Are The Symptoms & How Long Do They Last?” .
There is no conclusive evidence to suggest a significant difference in the withdrawal timeline between males and females. However, individual metabolism, body composition, and overall health influences the severity and duration of withdrawal symptoms. People with a history of substance abuse or high-dose methocarbamol use, experience more intense withdrawal periods.
To treat methocarbamol addiction requires a comprehensive approach that includes both medical and psychological support. The most effective treatments combine therapy, medication, and treatment at a specialized center, among other options.

The treatment options for methocarbamol addiction include:
Methocarbamol is not classified as a controlled substance by the U.S. Drug Enforcement Administration (DEA). It has a relatively low potential for abuse compared to other muscle relaxants or opioids. Despite this, methocarbamol still requires a prescription from a licensed healthcare provider due to potential risks of misuse, especially when combined with other CNS depressants like alcohol or opioids. It is FDA-approved and requires a prescription in the U.S., though in Canada, lower doses are available over-the-counter. According to the Anatomical Therapeutic Chemical (ATC) Classification System, it falls under M03BA (Carbamic acid esters).
Methocarbamol is used for relieving muscle spasms and pain, particularly in cases of acute musculoskeletal injuries such as neck pain, lower back pain, and sprains. It helps ease discomfort by acting on the central nervous system (CNS) to relax muscles indirectly, without directly affecting muscle tissue. Methocarbamol is prescribed for short-term relief and is used in conjunction with rest, physical therapy, and sometimes other medications like NSAIDs to maximize pain reduction and improve mobility during recovery.
The chemical composition of methocarbamol is C₁₁H₁₅NO₅, which is its empirical formula. It is classified as a carbamate derivative of guaifenesin, making it a centrally acting muscle relaxant with properties that depress CNS activity to reduce muscle tension and pain. This classification aligns methocarbamol with other skeletal muscle relaxants used for short-term pain management.
Robaxin-750 look like white, capsule-shaped tablets, while the 500 mg Robaxin tablets are light orange and round with a film coating. These formats allow for dosing adjustments based on patient needs and treatment plans.
Yes, you can overdose on Robaxin (methocarbamol) if you exceed the recommended dosage, which is generally 6 to 8 grams per day for short-term use. Taking amounts significantly above this range, especially 10 grams or more, increases the risk of severe side effects. The risk is even greater when Robaxin is combined with other central nervous system depressants, such as alcohol, opioids, or benzodiazepines, which amplifies the drug’s depressant effects on the brain and respiratory system.
If you take too much methocarbamol, it leads to symptoms of overdose, such as extreme drowsiness, dizziness, confusion, slow reflexes, and even loss of consciousness. Overdosing also results in respiratory depression, where breathing becomes dangerously slow or shallow, potentially leading to coma or death. Severe overdose cases require hospitalization and even death. Immediate medical attention to prevent life-threatening complications is necessary.
Yes, methocarbamol can cause an overdose if taken in excessive amounts. Muscle relaxants like methocarbamol, while generally less addictive than opioids, still lead to overdose when misused or combined with other CNS depressants. Overdosing on methocarbamol specifically affects the central nervous and respiratory systems, increasing the risk of fatal respiratory depression. From 2010 to 2020, there were 2,605 cases reported to the National Poison Data System and over half were suicide attempts.
The typical adult dosage of methocarbamol for oral administration averages 1500 mg, taken three to four times per day, for both men and women. This dosage is increased initially, where two 750 mg tablets (totaling 1500 mg per dose) are taken four times daily during the first 48–72 hours of treatment to establish muscle relaxation. After this initial period, the dose is typically adjusted to 1000 mg three or four times per day for ongoing relief.
Methocarbamol is also available in intravenous (IV) form for medical use in hospital settings, particularly for acute cases. For pediatric patients under 16, methocarbamol is not recommended, as its safety and efficacy in younger populations have not been fully established.
No, methocarbamol does not treat opiate withdrawal. First, it does not interact with opioid receptors, which are crucial for addressing opiate withdrawal symptoms. Second, while it provides relief for muscle spasms, it does not alleviate core withdrawal symptoms such as nausea, cravings, or psychological distress. Third, methocarbamol lacks the targeted effects of medications like buprenorphine or methadone, which are specifically designed to reduce opiate dependence and withdrawal symptoms.
No, methocarbamol does not make you high. It is designed to relax muscles rather than induce euphoria. Its action as a muscle relaxant does not affect dopamine levels, which are typically responsible for producing a high. Additionally, its calming effects primarily lead to drowsiness or mild sedation rather than euphoria, particularly at prescribed doses.
No, methocarbamol is not meth. "Meth" refers to methamphetamine, a powerful stimulant that is illegal in most contexts. Methamphetamine is known for its high potential for abuse and its intense stimulant effects on the central nervous system, leading to increased energy and euphoria. In contrast, methocarbamol is a CNS depressant, used medically to relieve muscle discomfort without the euphoric or stimulant effects associated with methamphetamine.
No, Robaxin (methocarbamol) is not a narcotic. It is classified as a muscle relaxant rather than a narcotic because it does not produce the intense pain-relieving effects or addictive properties associated with narcotics like opioids. Robaxin works by depressing the central nervous system to reduce muscle spasms but lacks the opioid-based mechanism and euphoria that narcotics induce.
No, methocarbamol is not a benzodiazepine. Methocarbamol is a muscle relaxant that primarily targets skeletal muscle discomfort, while benzodiazepines are a class of drugs that act on the central nervous system to relieve anxiety, insomnia, and seizures. While both have sedative effects, benzodiazepines affect the GABA receptors in the brain to reduce anxiety and induce relaxation, whereas methocarbamol’s action focuses on relieving muscle tension through CNS depression without significant anti-anxiety effects.
Yes, methocarbamol does interact with other medications, especially those affecting the central nervous system (CNS).
No, methocarbamol is not a strong muscle relaxer. It primarily works as a centrally acting muscle relaxant, indirectly reducing muscle spasms through CNS depression rather than directly affecting the muscles themselves. Compared to stronger muscle relaxants like baclofen or cyclobenzaprine, methocarbamol has milder sedative effects, making it more suitable for patients who need lower sedation levels. While higher doses (e.g., 1500 mg) increase its muscle-relaxing effects, it remains less potent than other muscle relaxants commonly prescribed for severe spasms.
No, methocarbamol is not a strong painkiller. It is classified as a muscle relaxant, so it addresses muscle pain indirectly by reducing spasms rather than providing direct pain relief. Methocarbamol lacks the analgesic properties found in NSAIDs or opioids, which target pain pathways. While increasing the dosage (such as up to 1500 mg) enhances its muscle relaxation effects, it does not increase its effectiveness as a painkiller.
No, methocarbamol is not a controlled drug. It is not classified by the DEA as a controlled substance because it has a low potential for abuse compared to drugs in the controlled categories, such as opioids or benzodiazepines. This classification applies to both methocarbamol and its brand version, Robaxin, allowing it to be prescribed without the strict regulations that apply to controlled substances.
What are the types of Methocarbamol Pills?
The types of methocarbamol pills available include various formulations distinguished by their markings, color, and dosage levels. Each pill type represents a specific appearance and identification code, helping to differentiate between manufacturers and strengths.
The types of methocarbamol pills include:
H 115 pill
B134 pill
G 500 pill
S226 pill
Orange G 750 pill
ASC 750 pill
G750 pill
G 500 orange pill
H 114 pill
By calling us, you agree to our Terms & Conditions
For those seeking addiction treatment for themselves or a loved one, our calls are confidential and are available for 24/7 help.
Any treatment center receiving calls from the site is a paid advertiser.
Calls to numbers on a specific treatment center listing will be routed to that treatment center.
Calls to any general helpline will be answered by treatment providers, each of which is a paid advertiser.
By calling the helpline you agree to the terms of use. These calls are offered at no cost to you and with no obligation to enter into treatment. Neither this site nor anyone who answers the call receives a commission or fee dependent upon which treatment provider a visitor may ultimately choose.
If you wish to explore additional treatment options or connect with a specific rehab center, you can: browse top-rated listings, visit our homepage, or visit SAMHSA, or by calling 800-662-HELP. You may also contact The Florida Department of Children and Family Services







